
 Parathyroid surgery is different from all other forms of human surgery because of the fact that there are four parathyroid glands. There are no other organs in the body that are present 4 times. The goal when performing parathyroid surgery is to remove only the bad parathyroid gland and leave the good ones. In about 70% of the time, its only one parathyroid gland that has become diseased (it grows into a benign tumor about the size of an olive or grape). The issue has always been that the surgeon doesn't know which parathyroid is bad--so they make a BIG operation to find all four glands. This operation is out-dated... do not do this. However, you DO want to have all four parathyroid glands checked by your surgeon, because if you don't 30% of you will need another operation in 10 years, 15% of you will need a second operation in 5 years. Watch this quick video of Dr Norman doing a minimally invasive 4-gland parathyroid operation in less than 13 minutes. This is very educational video and the operation you want! (there is no blood!)
Parathyroid surgery is different from all other forms of human surgery because of the fact that there are four parathyroid glands. There are no other organs in the body that are present 4 times. The goal when performing parathyroid surgery is to remove only the bad parathyroid gland and leave the good ones. In about 70% of the time, its only one parathyroid gland that has become diseased (it grows into a benign tumor about the size of an olive or grape). The issue has always been that the surgeon doesn't know which parathyroid is bad--so they make a BIG operation to find all four glands. This operation is out-dated... do not do this. However, you DO want to have all four parathyroid glands checked by your surgeon, because if you don't 30% of you will need another operation in 10 years, 15% of you will need a second operation in 5 years. Watch this quick video of Dr Norman doing a minimally invasive 4-gland parathyroid operation in less than 13 minutes. This is very educational video and the operation you want! (there is no blood!)
What is parathyroid anatomy? Where are parathyroid glands located?
Parathyroid anatomy is the most variable anatomy in the body. There are four parathyroid glands, two in the left side of the neck and two in the right side of the neck, located just behind the thyroid gland. The picture above and to the right shows the thyroid gland in the front of a patient's neck. The parathyroids are NOT related to the thyroid in function, but they are neighbors in the neck. The parathyroids are BEHIND the thyroid. The picture to the right shows a view of the BACK side of the thyroid. You can see that in most (but not all) people, there are two parathyroids behind each side of the thyroid. The parathyroids are shown in their normal 'mustard yellow' color. This picture also shows one big parathyroid adenoma (a benign parathyroid tumor) and three normal sized parathyroid glands. This is exactly what most people with parathyroid disease (hyperparathyroidism) have.
 Here is the biggest issue with parathyroid surgery, and why the experience of the surgeon is VERY important to the success of parathyroid operations: When the 4 parathyroid glands are formed (before we are born), they migrate from one part of the neck to another. THUS, they are not always were they are supposed to be! When you understand how the parathyroid glands are formed, you will understand why parathyroid anatomy is the most variable anatomy in the human body. The picture on the right shows that the parathyroid glands can be located from just below the jaw down to the area around the heart.
Here is the biggest issue with parathyroid surgery, and why the experience of the surgeon is VERY important to the success of parathyroid operations: When the 4 parathyroid glands are formed (before we are born), they migrate from one part of the neck to another. THUS, they are not always were they are supposed to be! When you understand how the parathyroid glands are formed, you will understand why parathyroid anatomy is the most variable anatomy in the human body. The picture on the right shows that the parathyroid glands can be located from just below the jaw down to the area around the heart.
Technically speaking, (stick with us here for just a minute) the four parathyroids arise from the third and forth branchial pouches. This means that they are formed early in embryogenesis along with other organs of the neck. The lower 2 parathyroids come from the third brachial pouch which is also responsible for producing the thymus gland (not thyroid) which is important for the development of a normal immune system. The thymus eventually sits behind the breast bone (sternum). The upper 2 parathyroids come from the fourth branchial pouch which also produces the thyroid gland.
Normally, as the larger thymus and thyroid glands migrate from the upper neck (where they are formed) into the lower neck and upper chest, they take the small "passenger" parathyroids with them. The lower parathyroids usually getting stuck in the neck next to the thyroid during this migration and rarely make it all the way into the chest with the thymus. Therefore, under normal circumstances, the lower parathyroids will usually be found just below and behind the bottom of the thyroid. BUT, they can be found behind the sternum (chest bone). Likewise, the upper parathyroids will be found behind the middle of the thyroid gland. That is to say, normally, all four parathyroids are found around the back side of the thyroid like in many of the pictures on this site.
BUT, it doesn't always go as planned !
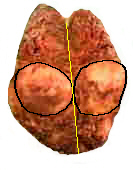 It is this migration of the parathyroid glands through the neck during our gestation in the womb that makes finding them tricky later in life. Occasionally, the upper parathyroid glands are formed with the thyroid to such a high degree that they never become separated. Under these circumstances, an upper parathyroid will actually be found INSIDE the thyroid gland. This picture shows the right half of the thyroid gland of a recently operated patient. I (Dr Norman) cut the thyroid in half to demonstrate the large parathyroid tumor (adenoma) which was inside the thyroid. The yellow line shows where I split the thyroid open and I have drawn a black line around the parathyroid tumor which was cut in half also.
It is this migration of the parathyroid glands through the neck during our gestation in the womb that makes finding them tricky later in life. Occasionally, the upper parathyroid glands are formed with the thyroid to such a high degree that they never become separated. Under these circumstances, an upper parathyroid will actually be found INSIDE the thyroid gland. This picture shows the right half of the thyroid gland of a recently operated patient. I (Dr Norman) cut the thyroid in half to demonstrate the large parathyroid tumor (adenoma) which was inside the thyroid. The yellow line shows where I split the thyroid open and I have drawn a black line around the parathyroid tumor which was cut in half also.
This young patient had primary hyperparathyroidism with a very high calcium and parathyroid hormone. The sestamibi scan showed that it was completely buried within the thyroid gland and the only way to adequately get the entire adenoma out and cure her disease was to remove the right lobe of the thyroid. Her remaining thyroid (the isthmus and left lobe) will make enough thyroid hormone so she will not have to take thyroid hormone pills. Keep in mind that this situation is uncommon (about 1 percent of all cases). But your surgeon should have enough experience and knowledge to deal with these difficult circumstances should they arise. This picture was taken after the specimen was in preservatives overnight (prior to being sliced and stained by the pathologist) that is why the colors have all turned brown.![]() Normally, the thyroid is a deep brown color and the parathyroid adenoma is a mustard yellow color. Even though the colors are not well preserved, you can easily see the large round parathyroid adenoma completely within the thyroid gland.
Normally, the thyroid is a deep brown color and the parathyroid adenoma is a mustard yellow color. Even though the colors are not well preserved, you can easily see the large round parathyroid adenoma completely within the thyroid gland.
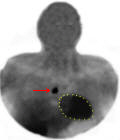 When the lower parathyroids fail to migrate normally, they can reside very high in the neck, several inches above the top of the thyroid. This is quite rare, but a very experienced surgeon should know this BEFORE they operate!! A more common parathyroid migration problem occurs when the lower parathyroids fail to separate from the thymus as the thymus makes its way to the chest to end up behind the sternum (although still uncommon, this happens in about 1% of patients with parathyroid disease). Instead of the parathyroids ending up just below the lower edge of the thyroid, they will go all the way into the chest and reside next to the heart. This picture shows just this case. There is a very "hot" parathyroid adenoma which shows up on this sestamibi scan just to the right of the patient's heart (the heart is outlined in yellow and the red arrow points to the parathyroid gland).
When the lower parathyroids fail to migrate normally, they can reside very high in the neck, several inches above the top of the thyroid. This is quite rare, but a very experienced surgeon should know this BEFORE they operate!! A more common parathyroid migration problem occurs when the lower parathyroids fail to separate from the thymus as the thymus makes its way to the chest to end up behind the sternum (although still uncommon, this happens in about 1% of patients with parathyroid disease). Instead of the parathyroids ending up just below the lower edge of the thyroid, they will go all the way into the chest and reside next to the heart. This picture shows just this case. There is a very "hot" parathyroid adenoma which shows up on this sestamibi scan just to the right of the patient's heart (the heart is outlined in yellow and the red arrow points to the parathyroid gland).
Once again, it is the migration of parathyroids which makes operating on them so tricky. This is one of the reasons that a number of surgeons believe that minimally invasive parathyroid surgery can be advantageous. With proper testing, a surgeon can tell BEFORE the operation where the overactive adenoma is located so so he/she doesn't have to search all areas of the neck. As discussed on a few of our other pages, sometimes these tests don't give any predictable information. BOTTOM LINE: An experienced surgeon can anticipate variances in anatomy before an operation.
One of the most important aspects of parathyroid surgery is that all four parathyroid glands must be examined if you expect to be cured long-term. Unfortunately, few surgeons can do this, so they rely on scans that are acurate about 70% of the time. If there is one thing that you learn from this page, it is that parathyroid gland anatomy is extremely variable and these little boogers can be located in MANY places in the neck (or chest). If there is a second thing you learn, it is that you want a surgeon who can find all four glands. Only taking out the gland that shows on a scan will mean that 30% of you will not be cured. Be smart, and keep reading!
If you like learning by watching videos, then look at the educational videos.
What to read next
- Hyperparathyroidism: The only disease of the parathyroid glands.
- The Signs and Symptoms of Hyperparathyroidism.
- Watch a minimally invasive 4-gland parathyroid operation performed in less than 13 minutes. A very popular and award-winning video.
- See more of our videos on one page... our Teaching Videos Page.
- Read the stories on our blog. Very Cool!
- See a Map of where our patients come from.
- How to become our patient